 Haemorrhoidectomy is the surgical resection of the haemorrhoids. General anaesthesia or raquianaesthesia is used to avoid pain. The incisions are performed in the tissue surrounding the haemorrhoids. The protruding haemorrhoid vein is ligated to prevent bleeding, and the haemorrhoid is excised. The surgical plague may be sutured or left open. Sterile dressing is applied onto the wound. The surgical intervention may be performed with a knife, a power tool (electrocautery tool) or using laser devices.
Haemorrhoidectomy is the surgical resection of the haemorrhoids. General anaesthesia or raquianaesthesia is used to avoid pain. The incisions are performed in the tissue surrounding the haemorrhoids. The protruding haemorrhoid vein is ligated to prevent bleeding, and the haemorrhoid is excised. The surgical plague may be sutured or left open. Sterile dressing is applied onto the wound. The surgical intervention may be performed with a knife, a power tool (electrocautery tool) or using laser devices.
There is a procedure using circular stapling to excise the haemorrhoids and suture the wound, without any incision. Through this procedure, the haemorrhoid is lifted and stapled back into the anal canal. This procedure is referred to as haemorrhoidopexy. People opting for this method may experience less pain than those opting for the traditional intervention, but it is, however, more costly and involves a higher relapse risk.
What to expect after the surgical intervention:
Recovery takes approximately 2-3 months. Immediately after the surgery, when you still are under the effect of the anaesthesia, you will be administered a local long-acting anaesthetic, which ensures a postoperative pain management of approx. 6-12 hours. If you are not admitted overnight, you will only be dismissed from hospital after the effect of the anaesthesia disappears and you urinate. Urinary retention may also occur as a consequence of an edema in the tissue or of a spasm in the pelvic muscles. We recommend that you ask someone to accompany you.
Postoperative care:
- you may feel pain after the surgery. If your physician recommended anti-inflammatories, please take them as prescribed. Ask your doctor what OTC drugs you should take;
- bleeding is a normal symptom, especially upon the first postoperative stool;
- in the first postoperative days, drink liquids and eat low fibre content foods (rice, bananas, toast, apple juice). After this period, you may resume your normal diet and gradually increase the fibre intake;
- you may use analgesics before and after the stool, to alleviate pain;
- ice packs in the anal area may help reduce swelling and pain;
- warm water sitz baths help alleviate pain and muscular spasms;
- some physicians may recommend antibiotics (such as metronidazole) after the surgery, in order to prevent infection and alleviate pain;
- physicians recommend laxatives to facilitate defecation. The pressure during defecation may cause haemorrhoid relapse;
- postoperative follow-up visits are generally performed after 2-3 weeks;
The necessity of the surgical intervention:
Haemorrhoidectomy is recommended for:
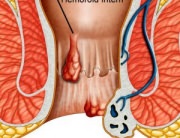
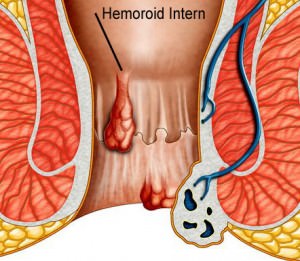
- very large internal haemorrhoids
- internal haemorrhoids with post-non-surgical treatment symptomatology
- large external haemorrhoids that cause significant discomfort and do not allow for proper local hygiene
- other haemorrhoid treatments (such as rubber band ligation) that had no results.
The efficiency of the surgical intervention:
Surgery generally cures haemorrhoids. The long-term success of the surgery largely depends upon the patients’ ability to change their diet and intestinal transit, so as to avoid constipation and defecation pressure. Approximately 15% of the cases relapse.
Risks:
Pain, bleeding and urinary retention are the most frequent secondary effects of haemorrhoidectomy.
Other relatively rare risks are:
- anal bleeding;
- accumulations of blood at the surgery site (hematoma);
- fecal and urinary incontinence;
- stool blocked on the anal canal (obstruction, occlusion);
- narrowing (stenosis) of the anal canal;
- haemorrhoid relapse;
- an abnormal passage (fistula) between the anal-rectal canal and another area;
- rectal prolapse, which represents the protrusion of the rectal mucous membrane through the anus.
Tips:
The success of the haemorrhoidectomy largely depends upon the patients’ ability to change their diet, in order to facilitate defecation. Haemorrhoidectomy may offer better long-term results than the procedures interrupting the blood flow towards the haemorrhoids (fixative procedure). The surgery is more expensive, it involves higher risks and it generally is more painful.
The condition of most internal haemorrhoids is improved (they become smaller and the discomfort disappears) through home treatment or modern therapies. As compared to the surgical intervention, modern treatment procedures involve a lower risk, less pain and require a shorter interruption of the daily activities or work. Surgical intervention is recommended for small internal haemorrhoids (only in the case of associated large internal haemorrhoids or internal and external haemorrhoids).
Laser treatments are recommended as fast healing and less painful alternatives, but neither of these statements is proven, and these methods also are more costly than the traditional ones. The procedure lasts longer and may cause tissue lesions.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}