 Approximately 90% of the women experience haemorrhoidal problems immediately after childbirth, a condition caused by the haemorrhoid disease. Haemorrhoids are defined as the clinical expression of the varicose dilations of the anal canal- and rectum-level veins. These veins enlarge because the blood backflow in the veins is hindered. Unfortunately, this richly represented circulation is against gravity. Sometimes, this adds to a nutrition deficiency leading to constipation, rectum irritation following the consumption of alcohol or excessive consumption of spices.
Approximately 90% of the women experience haemorrhoidal problems immediately after childbirth, a condition caused by the haemorrhoid disease. Haemorrhoids are defined as the clinical expression of the varicose dilations of the anal canal- and rectum-level veins. These veins enlarge because the blood backflow in the veins is hindered. Unfortunately, this richly represented circulation is against gravity. Sometimes, this adds to a nutrition deficiency leading to constipation, rectum irritation following the consumption of alcohol or excessive consumption of spices.
Pregnancy and childbirth generally exacerbate a pre-existing condition through the gradual increase in volume of the pregnant uterus and pursuant to the pelvic venous system compression effect. However, extensive sitting is, beyond doubt, the key cause. It is known as the clerks’ and drivers’ disease. The onset mechanism is very simple. The rectum is a flexible cylinder, which easily deforms under the pressure of the intraabdominal organs leading to the collapse of the vessels that circulate the peripheral venous blood. This leads to an increase in the haemorrhoidal system venous pressure, which accumulates in the rectal venous cushions and causes them to dilate.
The process generally is reversible up to a certain point. From there on, the integrity of the conjunctival system plays a key role, in that if we inherit a less elastic tissue, these vascular cushions do not return to their initial size after each increase in volume. The varicose vein dilations become larger and larger.
The only really wise thing to do is to make an appointment with a proctologist. You will receive expert advice regarding your lifestyle, your daily diet and, last but not least, an efficient treatment recommendation. Lately, we’ve been witnessing an increasing nuancing of the available therapeutic methods, ranging from the administration of local ointments, up to interventions that are easy to perform and well tolerated by the patient. The classical surgical intervention is now only reserved to the advanced forms of the disease or to the neglected, long-term evolving forms of the disease.
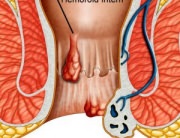
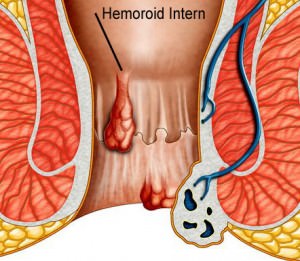
It should be explained that haemorrhoids are of two types, internal, which occur first, as varicose vein dilations, located in the crown, INSIDE the anal canal, approx. 4cm deep (responsible for the discomfort, bleeding and complications) and external haemorrhoids, which occur as a consequence of the decompensation of the venous drainage in the already dilated internal haemorrhoids. The latter have more of an aesthetic implication, being noticed by the patient, but they can also lead to complications in the case of the external haemorrhoid thrombosis, (an external haemorrhoid becomes thrombosed, there is a painful blue-ish tumefaction, on the edge of the anal canal).
The idea is that internal haemorrhoids are mainly responsible for the suffering, discomfort, bleeding, pain specific to the haemorrhoidal disease, even though the common, uninformed patient associates all these symptoms to external haemorrhoids.
Another myth to bust is that women experience haemorrhoids immediately after natural childbirth, and that their incidence is lower in the case of C-section. In fact, haemorrhoids grow out of venous lakes (haemorrhoidal plexus), present in all human bodies, under the form of venous cushions that ensure the natural sealing of the anal canal for gas. The venous drainage occurs NOT UPON CHILDBIRTH, BUT THROUGHOUT THE PREGNANCY, when there is venous compression on the lower cave tract, i.e., poor, delayed, prevented venous drainage, causes these venous cushions to gradually dilate, turning into haemorrhoids.
Childbirth, especially the natural one, also has an unfavourable influence on EXISTING HEMORRHOIDAL DILATIONS, because, during expulsion, it may cause the thrombosing of the haemorrhoids, leading to haemorrhoidal crises often interpreted by patients as incipient haemorrhoidal disease. It should be noted that all women can experience internal haemorrhoidal varicose vein dilations during pregnancy and immediately after birth. Some can improve with medicine treatment only, but in the case of a family history including varicose veins, hernias, haemorrhoids, flat foot or unfavourable professional conditions, such as lengthy sitting – jobs such as office clerk, driver, etc. – these dilations do not regress after the postnatal pelvic congestion period, but instead, they develop complications.
To conclude, post-childbirth haemorrhoids are a frequently encountered problem, and that is why all women experiencing anal discomfort after childbirth should request a proctology examination. In addition to the negative impact on the mother that recently went through the great but challenging experience of childbirth, they also indirectly REFLECT IN THE CHILD’S EVOLUTION, who may be put at risk, including through ablactation!
THE ABLACTATION THREAT INDUCES GREAT STRESS IN THE MOTHER, who, even though suffers from haemorrhoids, no longer contacts the physician, because she fears she could receive a medical treatment that is incompatible with breastfeeding. Completely wrong! Modern, easily tolerated treatments are currently available and LaurusMedical Clinics can provide those treatments.
Out physicians apply a modern treatment, relying on globally-recognized techniques, widely spread and appreciated in countries such as Germany, Italy, USA or UK. The clinic is equipped according to the strictest EU standards, combining state-of-the-art technology with an experience of more than 12 years of the medical personnel in the non-surgical haemorrhoid treatment. On the other hand, our physician staff includes consecrated surgeons, holding professional and didactic experience, which guarantees that the non-surgical treatment recommendation is knowingly made.
The treatment does not suppose hospital admission, it is performed in several sessions, at intervals of approximately 2-3 weeks, with minimum risks for the mother and the child. The sessions last for approximately 20 minutes. After the treatment session, the patient can return home and resume her everyday life, without bed rest or a medical leave, etc. The treatment is designed under the form of a package of services, which also includes critical haemorrhoidal disease investigations, such as rectosigmoidoscopy, in order to exclude other benign or malignant anal canal disease, performed by a GI medical specialist, with competency in lower GI endoscopy and abdominal ultrasound.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}