
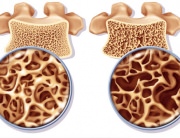
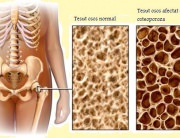
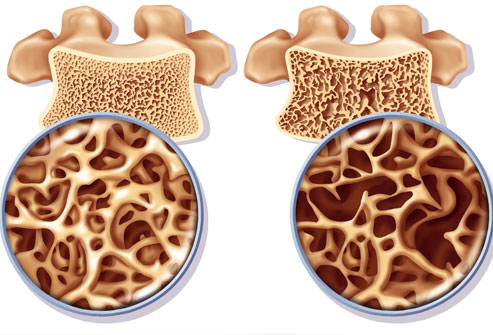
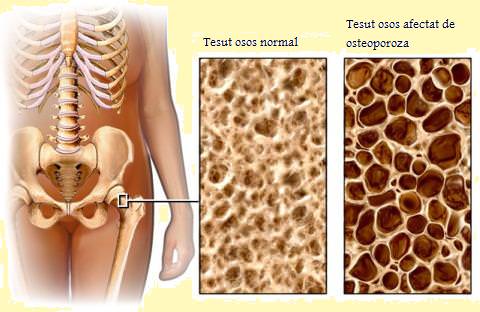
Osteoporosis (porous bone) is a condition that weakens the bones making them susceptible to fractures. Without prevention or treatment, osteoporosis may progress, without pain or symptoms, leading to bone fractures. These fractures most often occur in the hip and the spine. Osteoporosis causes more than 1.5 million fractures per year (300,000 hip fractures, 700,000 vertebral fractures, 250,000 hand joint fractures and more than 300,000 other bone fractures). In the US, the estimated yearly cost of treatment of osteoporosis and related lesions (hospitals and nursery homes) amounts to 14 billion dollars.
Even though have a higher predisposition to osteoporosis, the disease is not only encountered in elderly women. Osteoporosis is more frequent amongst white and Asian women above 50, but it may occur in any persons and at all ages. In fact, more than 2 million men in the US suffer from osteoporosis, whereas 3 million men feature an increased risk. Several people from the risk category or who suffer from osteoporosis are unaware that they have thin and fragile bones, because osteoporosis is asymptomatic before the fracture occurs. E.g.: a daily activity, such as lifting a shopping bag, can cause a bone fracture; slipping and falling onto the pavement can cause a hip fracture, and these are the first “symptoms”.
Osteoporosis generally is underdiagnosed in men because of several factors. Because osteoporosis can be largely prevented, the identification of risk factors is very important. The diagnosis of osteoporosis in men is also very important, because even though osteoporosis cannot be cured, it can be treated.
Why Is Osteoporosis Underdiagnosed in Men?
Large bone mass: Osteoporosis is mainly diagnosed in women, as they are more prone than men. However, “additional” protection against osteoporosis in men is temporary. This temporary protection is associated to the larger skeletal bones in men. Thus, men have larger bone mass reserves that they can use as they grow older, so the bone loss is slower. Moreover, men do not exhibit the sudden bone mass decrease that women experience during the menopausal and postmenopausal period.
Because of the delayed bone mass loss and of the absence of symptoms, men only realize that they suffer from osteoporosis when a bone fracture occurs. The raising of awareness of osteoporosis in men is essential to prevent it and protect long-term health.
Osteoporosis Test Standards:
Osteoporosis is diagnosed through the osteodensitometry test, which generally measures the bone strength and mass of the spine, hip and/or wrists (the bones that are most prone to osteoporotic fractures). These tests are performed just like X-rays and they are the safest method to calculate bone mass loss. The tests are safe, unpainful and non-invasive.
The osteodensitometry test results are compared to the reference values set based on a large population sample. One of the challenges of bone mineral density measurement in men is that the references used for comparison purposes were obtained in women, not in young men. The common bone mass in young healthy women always is lowered than the bone mass observed in young healthy men. Hence, a man may have a lower bone mass (osteopenia) as compared to healthy men, but the comparison to the reference (obtained in young women) will not identify the osteoporosis risk. As a consequence, fewer men are diagnosed with osteoporosis.
Osteoporosis and Fracture Risk Factors in Men:
Even though as compared to women the bone mass loss in men occurs later in life, they can be exposed to the same osteoporosis onset risk. By the age of 65, men reach the same bone mass loss rate as women. The additional risk factors such as the small body dimensions, the long-term use corticosteroids (prescription-based medication for a wide range of medical conditions: arthritis, asthma, Crohn’s disease, lupus or other diseases) or the low testosterone level (male sexual hormone) can increase the risk of osteoporosis in men.
It is estimated that by 2025, the overall number of hip fractures in men will be equal to that of hip fractures reported in women. Though men suffer from factures at an older age than women, they are generally more severely physically affected by the fracture. Just like in women, the bones that are most prone to fractures are the spine, the hip and the wrists. The complications and deceases caused by hip fractures in men are 3 times higher than in the case of women.
Male Bone Mass Loss and Fracture Risks include:
- certain types of medication (corticosteroids, anticonvulsants, heparin, excessive thyroid hormone replacement, certain cancer therapies);
- chronic diseases that affect the kidneys, the lungs, the stomach, the intestines and change the hormone levels;
- low testosterone levels;
- daily habits: smoking, insufficient calcium intake, insufficient exercising;
- aging
- hereditary factors;
- race (Caucasian men are most predisposed to osteoporosis. However, men of any race can develop osteoporosis).
Osteoporosis Screening in Men:
The early determination of the low bone mass (osteopenia) or of osteoporosis is the most important step in preventing and treating this disease. Even if the person already suffers from osteoporosis, measures can be taken to prevent the progressive bone mass loss. The prevention or treatment methods shall not be timely applied if the persons are unaware that they suffer from osteoporosis or if they fall under the high risk category.
The only way to measure bone strength are bone mineral density tests, which are similar to X-rays.
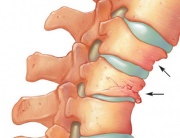
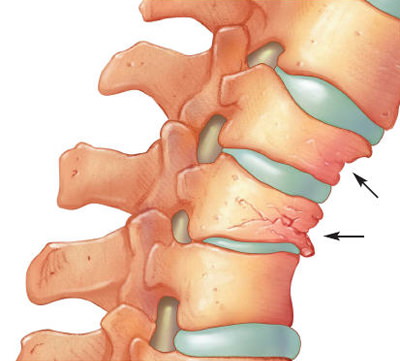
The physician must examine the medical history and identify the risk factors. Moreover, he must perform a full medical investigation, including the height and weight measurements, X-rays, urine and blood tests. Immediately inform your physician if you notice a height drop, a change in your body posture or sharp back pain, because these symptoms can indicate a vertebral fracture.
Osteoporosis Prevention in Men:
The development of the bones and the reaching of the maximum bone density (maximum strength), especially up to the age of 30, may be the best protection against osteoporosis. Moreover, a healthy lifestyle helps maintain the bone health, especially in persons above the age of 30. The medical research of osteoporosis in men is limited. However, experts agree that everyone should observe the same steps in order to maintain bone health.
All medical conditions that may affect bone health should be identified and treated. Moreover, the use of medication that causes bone mass loss should be identified and monitored. Give up bad habits, such as smoking. Start an exercising program. Make sure your daily calcium intake is of 1,000mg up to the age of 50 and of 1,200mg above 51. Make sure you have a proper vitamin D intake. Vitamin D can be obtained from two sources: through direct sun exposure and through diet. Many people naturally ensure the required vitamin D intake. Vitamin D is also present in dairy, egg yolk, salty water fish and liver. However, vitamin D production decreases with the age, in people immobilized at home and during winter. These people need vitamin D supplements to ensure a daily intake of 400-800 IU (international units).
Physical Exercising to Prevent Osteoporosis:
Physical exercises are an important osteoporosis prevention measure. Even though may seem as rough lifeless structures, they are similar to the muscle system; the bones are made up living tissue that reacts and is strengthened by physical exercise. Physical exercising during infancy and teenage increase the bone strength and density, and children who exercise a lot have great chances of reaching the maximum bone density (maximum strength and resistance). People reaching the maximum bone density, generally around the age of 30, are less prone to osteoporosis.
The most efficient exercises to prevent osteoporosis are antigravity exercises. Such exercises include walking, hiking, running, stair climbing;, tennis and dancing. The second type of exercises are strength exercises – activities that use muscle strength for the development of the muscle mass and of the bone strength. These activities include weight lifting using free weights or the devices in gyms. Physical exercising offers additional advantages amongst the elderly, because they increase muscle strength, the coordination capacity, the balance and boost wellbeing in general.
The elderly, people suffering from osteoporosis and people who have not regularly exercised should see a doctor before they start on an exercising program.
Osteoporosis Treatment in Men:
After you are diagnosed with osteopenia or osteoporosis, the doctor can inform you on the medication used to treat bone mass loss. The purpose of the treatment is to prevent aggravation of osteoporosis (if a low bone mass or other risk factors are identified) and the progressive mass loss (especially in the case of an osteoporosis diagnose). The final purpose is to maintain the current bone mass and density, to reduce the risk of osteoporosis fractures and disabilities. It has been shown that most current treatments quickly act (within no more than one year) and they lower the osteoporosis fracture risk by up to 50%. The selected treatment must suit your medical needs and lifestyle, so it is important that you contact a doctor.
Alendronate (Fosamax) is a drug approved for the treatment of osteoporosis in men. Alendronate and Risedronate (Actonel) are approved for the treatment of steroid-induced osteoporosis – the consequence of the long-term use of steroids such as prednisone or cortisone.
Strontium ranelate (Osseor) is a state-of-the-art drug, acting on the bone through a completely different mechanism than that of bisphosphonates. It boost bone formation, while also reducing bone resorption and thus rebalances the bone metabolism. Hence, strontium ranelate increases the bone mass, while also improving the bone micro-architecture. It is administered daily, approximately 2 hours after the evening meal.
Even though many drugs are prescribed to treat osteoporosis in women, they are not yet approved for use in men, but experimental trials in men are ongoing. In order to help men suffering from osteoporosis and a low testosterone level, doctors may recommend testosterone replacement therapies. In men, testosterone causes a reduced, but significant bone density increase.
Calcitonin is another drug that reduces or stops bone mass loss and can relieve pain in patients with fractures. The drug is approved for the treatment of osteoporosis in postmenopausal women. Even though its effects in men have not been studied, proof suggests that this drug has the same effect in both women and men. It is available in injectable format and as nasal spray.
Teriparatide (Forteo) contains a fragment of the parathyroid hormone (parathormone) molecule and has shown spine bone density increase in men. It is administered daily, in injectable format and it used in men suffering from hypogonadal osteoporosis (low testosterone level).
Sodium fluoride is a drug currently pending research.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}