Patient information on the risks associated to proctological disorders. The latest proctology news, new diagnosis and treatment methods.
Overview of External and Internal Haemorrhoids
Haemorrhoids are defined as the clinical expression of the varicose dilations of the anal canal- and rectum-level veins. These veins enlarge because the blood backflow in the veins is hindered. Unfortunately, this richly represented circulation, is against gravity. Sometimes, this adds to a nutrition deficiency leading to constipation, rectum irritation following the consumption of alcohol or excessive consumption of spices.
Pregnancy and childbirth generally exacerbate the pre-existing condition through the gradual increase in volume of the pregnant uterus and pursuant to the pelvic venous system compression effect.
However, extensive sitting is, beyond doubt, the key cause. It is known as the clerks’ and drivers’ disease. The onset mechanism is very simple. The rectum is a flexible cylinder, which easily deforms under the pressure of the intraabdominal organs leading to the collapse of the vessels that circulate the peripheral venous blood. This leads to an increase in the haemorrhoidal system venous pressure, which accumulates in the rectal venous cushions and causes them to dilate. The process generally is reversible up to a certain point. From there on, the integrity of the conjunctival system plays a key role, in that if we inherit a less elastic tissue, these vascular cushions do not return to their initial size after each increase in volume. The varicose vein dilations become larger and larger.
The only really wise thing to do is to make an appointment with a proctologist. You will receive expert advice regarding your lifestyle, your daily diet and, last but not least, an efficient haemorrhoid treatment recommendation. Lately, we’ve been witnessing an increasing nuancing of the available therapeutic methods, ranging from the administration of local ointments, up to interventions that are easy to perform and well tolerated by the patient. The classical surgical intervention is now only reserved to the advanced forms of the disease or to the neglected, long-term evolving forms of the disease.
Haemorrhoids are vein cushions located inside and around the rectum. When the inflame, they can cause itching, pain or bleeding. Unfortunately, haemorrhoids only get worse with time, never better. That is why we recommend a safe, bearable and efficient haemorrhoid treatment, as soon as their presence is noted.
Internal haemorrhoids are located upper on the anal canal, they’re not visible. Bleeding is the most commonly encountered and often the only internal haemorrhoid symptom. External haemorrhoids are visible outside the anal canal. Haemorrhoids actually are veins located under the skin, which become swollen and blueish. These haemorrhoids appear without any symptoms. However, once they inflame, these haemorrhoids appear red and sensitive.
Sometimes, internal haemorrhoids come out of the anal canal, a phenomenon referred to as haemorrhoidal prolapse; it is very difficult to reinsert them back into the anal canal and usually are very painful.
When a blood clot forms inside an external haemorrhoid, a sharp pain is generally resented. These thrombosed haemorrhoids appear in the anal area like hard peas.
Transabdominal Ultrasound
Just like all medical imaging methods, ultrasound has its plus and minuses, helping to exclude or confirm a certain diagnosis. Even though its role is limited to the diagnosis of digestive tract conditions, over the past years, due to the improvement of the US devices (new software, with real-time 3D-4D or sonoCT techniques) spectacular digestive tract images have also been obtained.
The importance of transabdominal digestive tract US is often underrated in clinics. This is due to the sonographic presentation of the digestive tract segments from an anatomic point of view (e.g., the back wall is hard to view because of the gas bubbles inside it). There are certain diseases where US plays a key role: intestinal obstruction, appendicitis, diverticulitis, Crohn’s disease. However, this very much depends on the experience of the operator, the imaging specialist. Moreover, it also helps obtain a real-time diagnosis, with minimum traumas or secondary effects for the patient, especially if the patient is a child or a pregnant woman.
Except for emergencies, a certain training is requested for ultrasound, required in order to obtain a suitable sonic window, with the avoidance of the artefacts generated by the presence of gas, food residues or the increase of the digestive tract lumen discharge (e.g., the presence of the fluid inside the intestine may be a sign of obstruction, inflammatory disease or malabsorption).
The ultrasound examination is performed after a period of rest of approx. 4-6 hours. This does not apply in the case of patients suffering from diabetes mellitus. In this case, a light breakfast is allowed! The examination is performed using a 3-5Mhz frequency probe. 5-10Mhz probes can be used in children or low weight patients, especially if there is a prior diagnosis.
Anatomically, the digestive tract has 5 layers. The thickness of the wall varies: from 5mm (gastric antrum – horizontal section of the stomach) to 1-2mm (duodenum and small intestine). At the level of the colon, the thickness is of approx. 3mm, and in case the colon is filled with air and distended, its size importantly decreases. The width of the digestive tract lumen varies a lot – in the small intestine it is of less than 2cm.

Colonoscopy to Diagnose Colon Cancer
The patient with a proctologic condition comes to the doctor’s practice for bleeding through the anal orifice (red blood, generally accompanying the stool or not), ano-perianal pain with various degrees of severity (discomfort, stinging, pain), haemorrhoid prolapse (reducible or not). Following the discussion with the patient (anamnesis and medical history) and the clinical examination (which, in this case, includes the digital rectal examination and the anoscopy), the doctor sets a stage diagnosis. It must be supported by further investigations (positive diagnosis) and each of the patient’s symptoms must be analyzed in terms of the condition triggering it (differential diagnosis).
It is important that the differential diagnosis is set based on all the signs and symptoms determining the patient to request a specialist consultation. Red blood leakage through the anal orifice can be triggered by a proctologic disorder (haemorrhoids, anal fissures), excluding a hemorrhagic risk condition on the rectum or left-hand side colon. In this respect, a rectosigmoidoscopy is recommended, as it may highlight disorders such as: colon polyps sau polyposis, colon diverticulosis, colon cancer, inflammatory colon diseases (ulcero-hemorrhagic rectocolitis, Crohn’s disease, indeterminate colitis), angiodysplasia injuries.
Haemorrhoids After Childbirth
Approximately 90% of the women experience haemorrhoidal problems immediately after childbirth, a condition caused by the haemorrhoid disease. Haemorrhoids are defined as the clinical expression of the varicose dilations of the anal canal- and rectum-level veins. These veins enlarge because the blood backflow in the veins is hindered. Unfortunately, this richly represented circulation is against gravity. Sometimes, this adds to a nutrition deficiency leading to constipation, rectum irritation following the consumption of alcohol or excessive consumption of spices.
Pregnancy and childbirth generally exacerbate a pre-existing condition through the gradual increase in volume of the pregnant uterus and pursuant to the pelvic venous system compression effect. However, extensive sitting is, beyond doubt, the key cause. It is known as the clerks’ and drivers’ disease. The onset mechanism is very simple. The rectum is a flexible cylinder, which easily deforms under the pressure of the intraabdominal organs leading to the collapse of the vessels that circulate the peripheral venous blood. This leads to an increase in the haemorrhoidal system venous pressure, which accumulates in the rectal venous cushions and causes them to dilate.
Colon Polyps
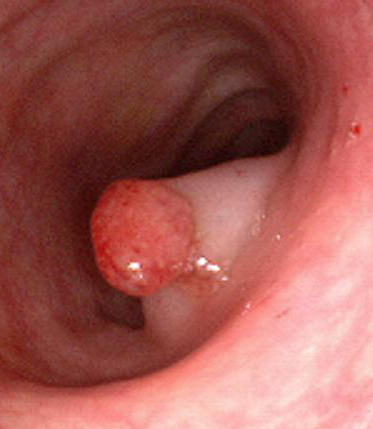
Colon Polyps are clearly delimited growths (protrusions), developed at the level of the colon mucosa. These lesions are very important, because they are regarded as pre-cancerous growths, responsible for most colorectal cancer forms. The identification and endoscopic resection of these lesions, as well as the patients’ follow-up, decrease or even remove the individual colorectal cancer risk. Colon polyps vary in shape, size and location.
They can be sessile, with a wide implantation basis or pedunculated, with a pedicle (foot) that links the polyp head to the colon wall. Depending on their size, they can be small (below 5mm), average (5-15mm) and large (above 15mm), the latter featuring a high malignant transformation risk. Polyps can occur anywhere at the level of the colon, but there is, however, a predisposition for the left (descendent, sigmoid) colon in 70% of the cases. Hence, flexible rectosigmoidoscopy is an excellent and cost-efficient method to detect these lesions.